Local anesthesia and mild sedation.
Walking to and from the operating room.
Gasless laparoscopic sterilization using an amnioscope. Video
Acta Obstetricia et Gynecologica. 2010; 89: 975–979
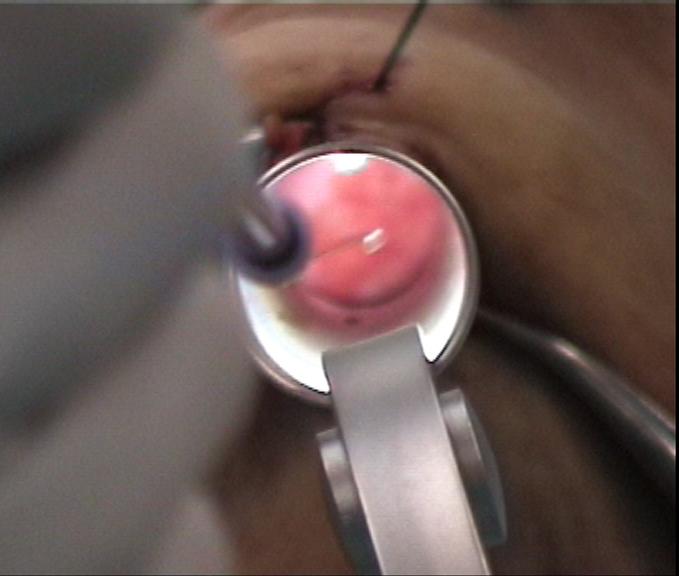
This new procedure is very similar to female sterilization by suprapubic minilaparotomy technique, using retractors. An amnioscope is in fact a tube formed retractor and in the gasless laparoscopic technique, it is used to keep the incision open, to pull (lift) and for direct visual inspection and instrumentation. The amnioscope is placed through a subumbilical incision (1,5-2 cm) and the amnioscope/abdominal wall complex is lifted with a loop suture (e.g. PDS # 1) snared around the shaft of the amnioscope with a hang knot and needle driven through the fascia, cutaneous tissue and skin in the lower end of the abdominal wall incision. The loop suture is attached to a horizontal metal arm mounted on the operating table and placed above the woman – e.g. an ordinary anesthesia frame with the horizontal arm draped in a sterile sleeve. Lifting the skin and subcutaneous tissue 6–8 cm above the symphysis pubis in the same way, using a towel clamp, optimizes the intraabdominal space formation.
The differences between minilaparotomy and the amnioscope lifting technique are a smaller incision (improvement), a retractor that by its tubular form hinders the intestines to block the sight (improvement) and a visual distance that is 10 cm longer, which is an improvement because the surgeon gets more of a “panorama” like view and thus a much better inspection of the pelvic organs. Moreover, at umbilicus, the abdominal wall is thinner than suprapubically and a smaller incision gives an aesthetically more acceptable scar, a shorter recovery period and less complications/complaints.
The resemblance with minilaparotomy is striking if the amnioscope lifting technique is compared with post-partum subumbilical minilaparotomy. In both procedures, retractor(s) are used to enable direct visual inspection, instrumentation and lifting.
Gasless laparoscopic sterilization under local anesthesia and mild sedation, in an office setting, using an amnioscope for inspection, instrumentation and lifting, is an arrangement between the best parts of conventional laparoscopy and minilaparotomy and it conforms well to the statement of the WHO Task Force on Female Sterilization (1982). “The ideal female sterilization would involve a simple, easily learned, one-time procedure that could be accomplished under local anesthesia and involve a tubal occlusion technique that caused minimum damage. The procedure would be safe, have high efficacy, be readily accessible, and be personally and culturally acceptable. The cost for each procedure would be low and there would be minimal costs for the maintenance of equipment”.
Woman in developing countries, where suprapubic minilaparotomy is a common approach and resources are limited for the purchase and maintenance of more sophisticated laparoscopic equipment, would probably benefit from this truly cheeper and safer "amnioscope-lifting" procedure.
Padded shoulder supports are an important prerequisite, because if a woman slides downwards on the table she gets scared and tense her abdominal muscles to stay put. This tends to press the intestines into the pelvis. Therefore, shoulder supports convince the woman that she will not fall to the floor. There is no risk of shoulder pressure injuries because the woman is awake and able to adjust to a comfortable position. However, despite the shoulder supports it is necessary for the woman to lie with her pelvic region 10 cm outside the table. This position gives necessary sliding distance to prevent the Hulka forceps from being blocked by the table when it is placed in the steep Trendelenburg position.
Before ligation, the isthmic part of the Fallopian tube is sprayed with the local anesthetic solution and after one-minute rest, infiltrated with the same solution using a long needle instrument.
The combination of mechanical lifting with passiv room air filling, the Trendelenburg position and the forward rotation of the uterus creates adequate intraperitoneal space to identify, anesthetize and ligate the tubes (rings, clips or diathermy).
Women experience the lifting procedure like being "lifted in the pants".
Only fluid food intake the day before surgery and a microlax enema the same morning, optimize the intra-abdominal free space formation.
Simplicity & Quality
|